The James B. Coakley Medal: Dissecting An Extraordinary Experience
Ning Xuan Ho, UCD School of Medicine, University College Dublin, Belfield, Dublin 4
Dr Michelle L. Smith, UCD School of Medicine, University College Dublin, Belfield, Dublin 4
The James B. Coakley Medal in Dissection is an annual dissection competition in University College Dublin (UCD) which takes place during the summer months. James B. Coakley was a professor of Anatomy in UCD from 1962 – 1988. To honour his distinguished career and his dedication to excellence in the teaching of human anatomy, the Coakley Medal is awarded to a current student based on exemplary dissection of an assigned specimen.
I applied to take part in the 2015 competition, with the application process beginning in May. After the application forms were submitted and reviewed, candidates were selected based on academic performance. Myself and three other candidates, Esther Shan Lin Hor, John Harford and Michael Gilligan were chosen to compete for the medal. Once notified, we were offered four projects to choose from and asked to list them in order of preference. The projects were then allocated according to GPA ranking. By good fortune we each ranked different projects highly and were therefore allocated our first choice, as follows:
• Dissection of the central visual pathway – Michael Gilligan
• Superficial and deep dissection of the knee – Esther Shan Lin Hor
• Dissection of pelvic topography – John Harford
• Dissection of the structures of retroperitoneum – Ning Xuan Ho
“the quality of our dissections, the educational value of our posters and the quality of our oral presentations”
The competition involves judgment of three components: the quality of our dissections, the educational value of our posters and the quality of our oral presentations. Prior to commencing the competition we each submitted a proposal outlining how we would approach the dissection. After a discussion with each participant, Doctors Feeney and Smith offered feedback and guidance for our dissection technique. We were also invited to attend an induction and photography technique session held in the human anatomy dissection laboratory which proved useful.
The dissection component of the competition took place from early July to late August. During this period, participants were notified of the days during which they would be afforded access to the human anatomy laboratory to perform dissection. Upon completion, the resulting specimens were assessed by a panel of academic staff from the Department of Anatomy at UCD.
Although we were allowed access to the dissection room from the first week of July, I commenced my project towards the end of July due to other commitments. However, my advice for future participants would be to start their projects early to get the best out of the competition. Upon completion of the dissection, it was time to design and complete our posters. My poster focused mainly on the photographic representation of my project and some discussion of the related anatomy. I also chose to feature some of the anomalies encountered during the dissection. However, there were no strict guidelines for poster content, and participants are encouraged to be creative in this aspect of the competition. We were permitted one week to complete the poster, which was reviewed by the academic staff in a digital format. The oral presentation took place at the beginning of the academic year. We gave a presentation containing images of our prosections to other students, anatomy demonstrators and professors. I found this experience quite daunting, however I enjoyed the novelty and excitement associated with communicating about my medical endeavors to an audience of my peers and mentors.
“My project became even more interesting as I discovered several anatomical anomalies”
I had a number of reasons for opting to dissect the retroperitoneum. First, I had recently completed a module on renal biology, and the concept of the retroperitoneum was still fresh in my mind. I thought this project was a good opportunity for revision, as well as a chance to gain a better understanding and appreciation of the area. Second, I believed that due to the depth of the retroperitoneal structures, I would encounter a wealth of anatomy as my dissection progressed from superficial to deep structures. I anticipated having the opportunity to examine the structures of the anterior abdominal wall and each of the intra-abdominal organs as I progressed with my dissection. As it developed, my project became even more interesting as I discovered several anatomical anomalies and pathologies.
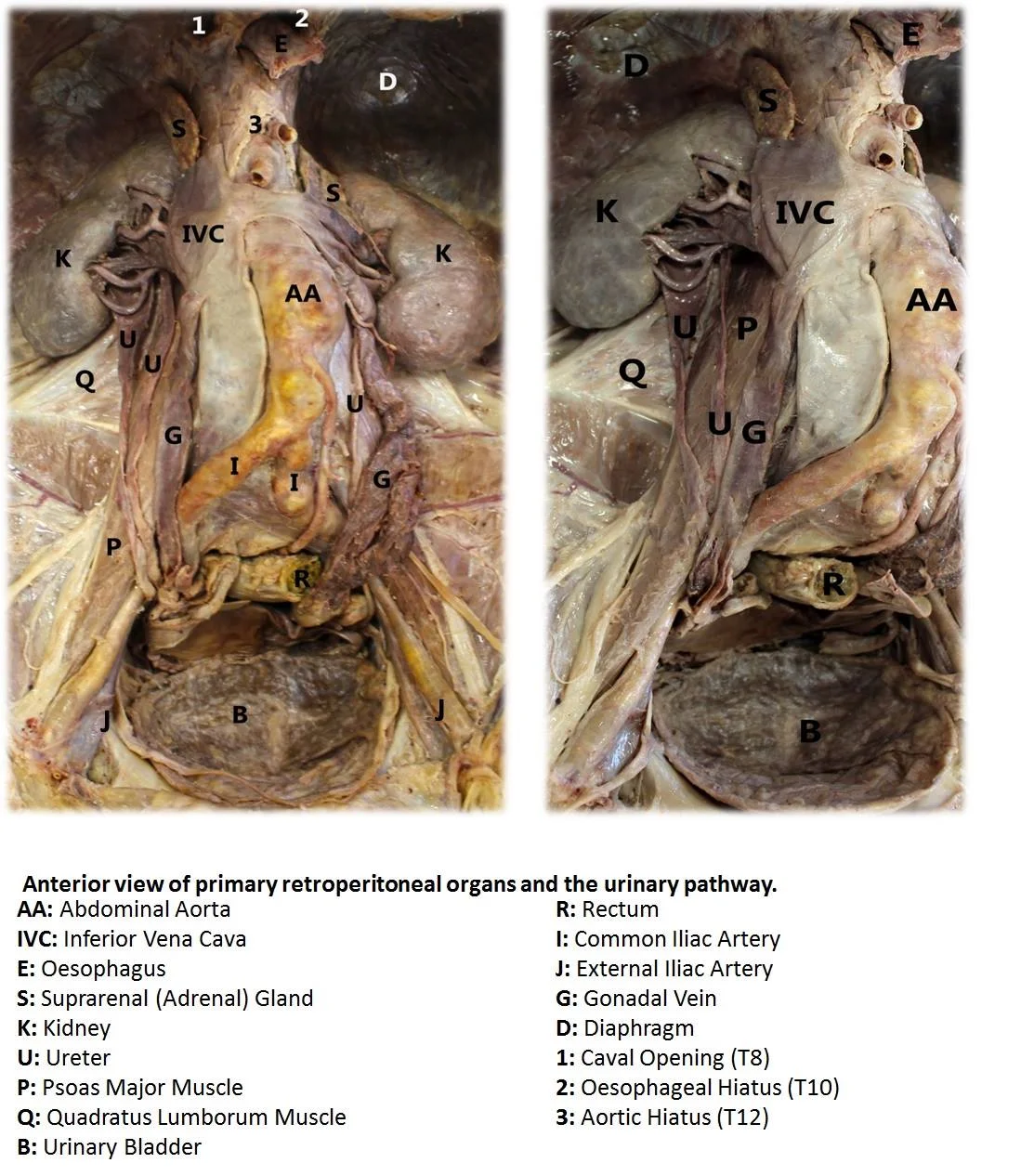
In my approach to this dissection, I began by identifying and marking the surface anatomy prior to making an incision. Once I had verified that the markings were correct, I incised the anterior abdominal wall, revealing the contents of the abdominal cavity. After examining the complex structure of the peritoneum and the mesentery, the peritoneal viscera were carefully removed. Following this step, the structures of the retroperitoneum were exposed. Using the camera provided, I took photographs at every stage of my dissection. This enabled me to document my progress and ensure that I had a record of all of the structures I encountered This photographic record proved useful for my poster and oral presentation.
“At this point I noticed a duplicate ureter emerging from the right kidney”
Moving on to the retroperitoneum, I exposed the kidneys and the path of the ureters. At this point, I noticed a duplicate ureter emerging from the right kidney. This is one of the more commonly described congenital anomalies, and is referred to in medical literature as a “duplex renal system”. Embryologically, this phenomenon occurs when two ureteral buds arise from the mesonephric duct during development. The pattern of duplication can vary. In this case, two completely separate ureters drained the right kidney. This system is seen in 0.7% of the normal adult population and in 2-4% of patients investigated for urinary tract symptoms.[1]
Duplex renal systems usually do not require any treatment per se, however complications may necessitate intervention. Duplicated ureter is reportedly more common in females compared to males. However, this may reflect more frequent investigation of the female urinary tract owing to their higher susceptibility to urinary tract infections, rather than a true increased frequency of this anatomical anomaly.[2] Duplicate ureters are usually discovered incidentally post-mortem, as was the case with our donor. Fascinated by this finding, I further examined the kidney by making a coronal section from the medial to the lateral surface. I discovered two completely separate renal pelvises, where the upper pole system was slightly smaller than the lower pole.
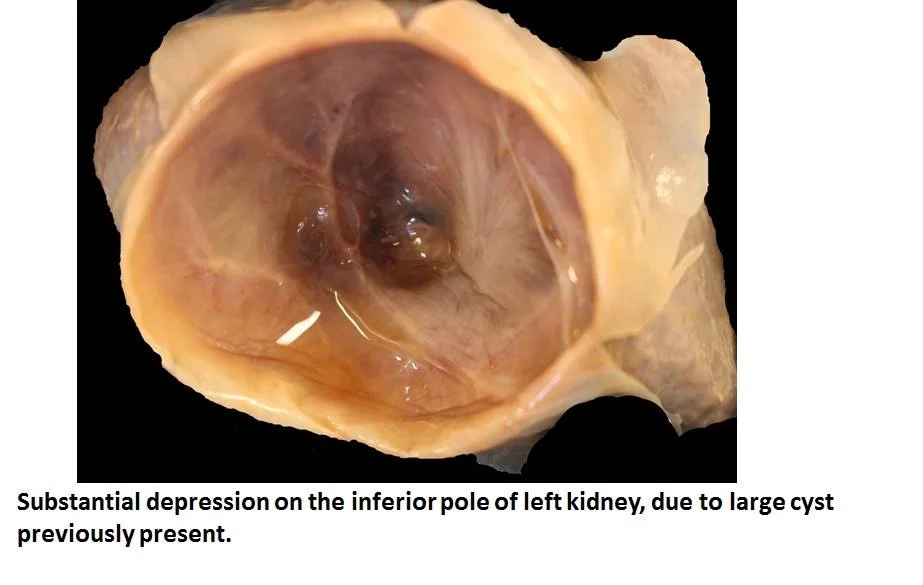
“The cyst measured approximately 50mm in diameter”
Next, I examined the left kidney. As I removed the pre-renal fascia I palpated an area with a much softer texture than the surrounding tissue. Upon exposing the renal capsule, I noted a cystic structure on the inferior pole. After draining off the fluid within this structure, there was a substantial depression on the antero-inferior and posterior segments of the kidney. We concluded that this was likely to be a simple cyst. Simple renal cysts are relatively common and measure approximately 10- 50 mm in diameter, with some measuring up to 100 mm. In this case, the cyst measured approximately 50 mm in diameter. Simple renal cysts are a common post-mortem finding. They are usually asymptomatic and have no clinical significance.[3] The function of the glomeruli which are compressed by the cyst may be impaired or obliterated, however due to the large reserve of filtering tissue in the kidney, this would not necessarily affect renal function.
Some intra-abdominal anomalies and pathologies were discovered during the dissection. First, the donor had an enlarged and discoloured liver with a grossly abnormal appearance. This was an interesting finding and a great learning point for all those involved in the competition, as we tried to correlate the observed anatomy with the pathology covered in lectures. As the dissection progressed, we noted various other pathological findings, including splenomegaly, severely calcified arteries and a large thrombus within the left ovarian vein. Collectively, these findings suggest the donor may have had portal hypertension. Unfortunately, we did not have access to medical records to confirm or refute this diagnosis.
“I have learned to appreciate both normal and variant anatomy, as well as pathological appearances”
Another interesting anomaly in the peritoneal region was a ‘splenunculus’. This appeared as a small, solid mass measuring approximately 20 mm in diameter. It was located just below the inferior pole of the spleen and covered by peritoneum. The splenunculus appeared to have its own local blood supply upon removal of the peritoneum. At first I wasn’t certain what it was, and sought the opinions of various anatomy lecturers. Following histological analysis, it was identified as splenic tissue. This demonstrates that learning human anatomy is not merely about appreciating the structures as ‘text book’ specimens, but that fascinating variations are also possible. Over the course of my project, I have learned to appreciate both normal and variant anatomy, as well as pathological appearances.
A significant amount of preparation was required in advance of beginning the dissection. I relied heavily on Grant’s Dissector,[4] which I found to be an extremely helpful and reliable resource. For students involved in this competition in future, I recommend visiting the library and examining a number of different atlases, texts and dissection guides, as certain books will vary in their suitability for particular dissections. I recommend that prospective Medal students make use of the allocated practical sessions to hone dissection skills. As I was working through my project, it took time to grasp certain techniques and to master the use of different dissecting tools to prevent damaging the tissues. However, after some practice, my dissection proficiency improved as I became more experienced and confident with the tools.
“I would definitely consider surgery as an option in the future”
Although I did not win the medal in 2015, I must say that this was a one-of-a-kind experience and I have gained so much more than I expected. My interest in a surgical career was certainly strengthened by participating in this competition and I would definitely consider surgery as an option in the future. The skills obtained and knowledge acquired were a huge part of what made this project worthwhile. Through this competition, I was able to develop my dissection skills, investigate several anatomical anomalies, as well as interact with various health science academics. I also had the opportunity to deliver an oral presentation to my peers and mentors, which although daunting at first, was a very rewarding experience. These are just some of capabilities I have developed during the competition. If asked would I do it all over again, my answer would be a resounding “Yes! Most definitely!”
ACKNOWLEDGEMENTS
I’d like to express my sincere gratitude to the donors and their families for the sacrifice that they make in order for this project (and all anatomical dissection at our medical school) to be possible. I would also like to thank the anatomy technicians, demonstrators and faculty of the School of Medicine for the valuable advice given throughout the project. Last but not least, to my fellow participants; John, Esther and Michael, thank you for making the dissection sessions so enjoyable and motivating. Finally, congratulations to Michael Gilligan on winning the 2015 James B. Coakley Medal in Dissection!
For those who are interested, students who have completed one year of Anatomy are eligible to apply to take part in the James B. Coakley Medal in Dissection. This includes students in undergraduate and graduate entry medicine, BHLS, radiography and physiotherapy programs. Further information will be posted on Blackboard in the coming months.
References
1. Hacking, C and Jones, J et al. Duplex Collecting System. Radiopaedia.org (http://radiopaedia.org/articles/duplex-collecting-systemhttp://radiopaedia.org/articles/duplex-collecting-system)
2. Gatti, J.M., Koo, H.P., Williams, J.F., Murphy, J.P., Ureteral Duplication, Ureteral Ectopia, and Ureterocele (September 2013) (http://emedicine.medscape.com/article/1017202)
3. Kumar, V., Abbas, A.K., Aster, J.C. Robbins and Cotran Pathologic Basic of Disease (9th ed.)
4. Tank, P.W. Grant’s Dissector 15th edition. 2013. Chapter 4: The Abdomen.